
Get Lit
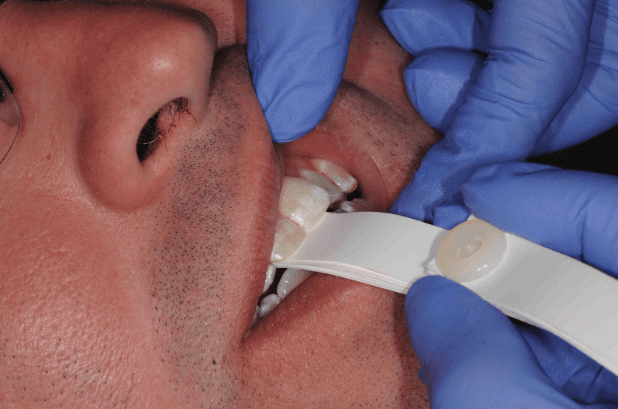
When Your Occlusal Clearance Disappears
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org It can be an incredibly frustrating clinical situation…
An Occlusion-Focused Hygiene Exam
By: Bill Gregg DDSTopic Originally Appeared on PankeyGram.org During an occlusion-focused hygiene exam, there are certain things…
Why Study Occlusion?
By: Kevin Muench DMD, MAGDTopic Originally Appeared on PankeyGram.com I’m a restorative dentist with a passion for…
Dr. Sable Muntean Appointed as Chief Editor of Get Lit Newsletter
Get Lit Newsletter Welcomes Dr. Sable Muntean as Chief EditorIgniting Success for New Dentists with Enhanced Content…

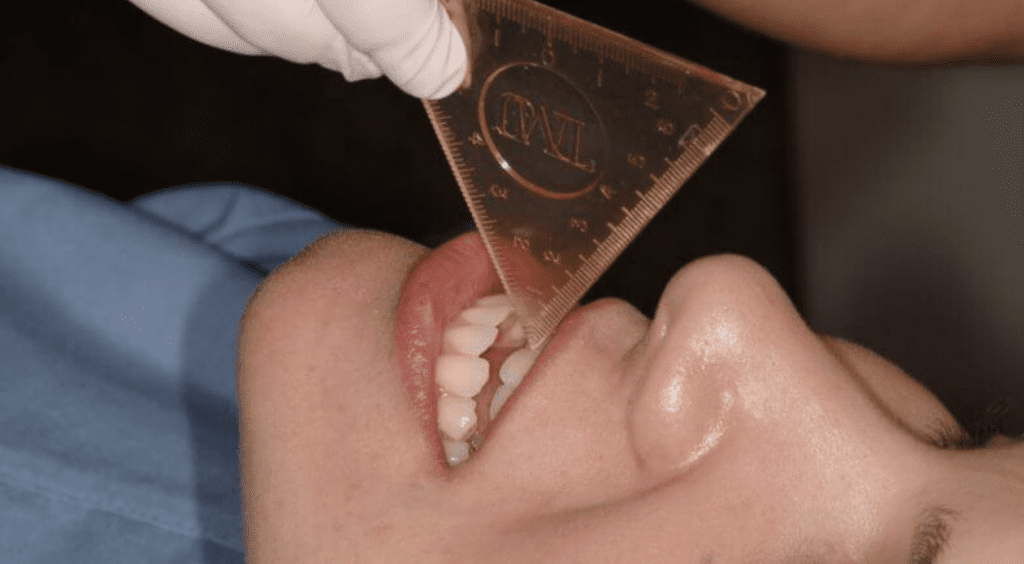
Occlusal Wear: Is It Advancing? How Fast?
By: Lee Ann Brady DMD I ask the question “Is wear normal?” at almost every lecture I…

How to Best Work with Patients on Clear Aligners
By: Allison Lacoursiere Clear aligners have made themselves incredibly important to our industry in a very short…

Misconceptions about Dental Insurance
By: Teresa Duncan One of the big issues that new dentists face is learning the ins and…

What’s Keeping You From Being Good Rather Than Great?
One degree can make the difference betweenwater boiling and just being really hot. I know a lot…

4 Principles to Grow Your Dental Practice
By: Dr. David Rice “Mask Mouth”. What does that mean for your dental practice? Let’s be honest….

Wildfires and another link between the mouth and lungs
The devastating wildfires in the United States are all over the news and likely on the minds…