
![]()
Dr. Lee Ann Brady lives in Phoenix, Arizona with her husband Kelly and three children Sarah, Jenna and Kyle. She owns Desert Sun Smiles Dental Care, a private restorative practice in Glendale, Arizona. Outside of her private practice, Dr. Brady is the Director of Education for The Pankey Institute, recognized for hands-on education programs focused on occlusion and restorative dentistry. She is the founder and lead curator of Restorative Nation, a supportive learning community for dentists.
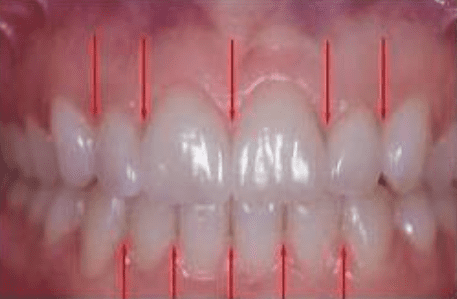
Interdental Papilla: Esthetic Considerations
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…

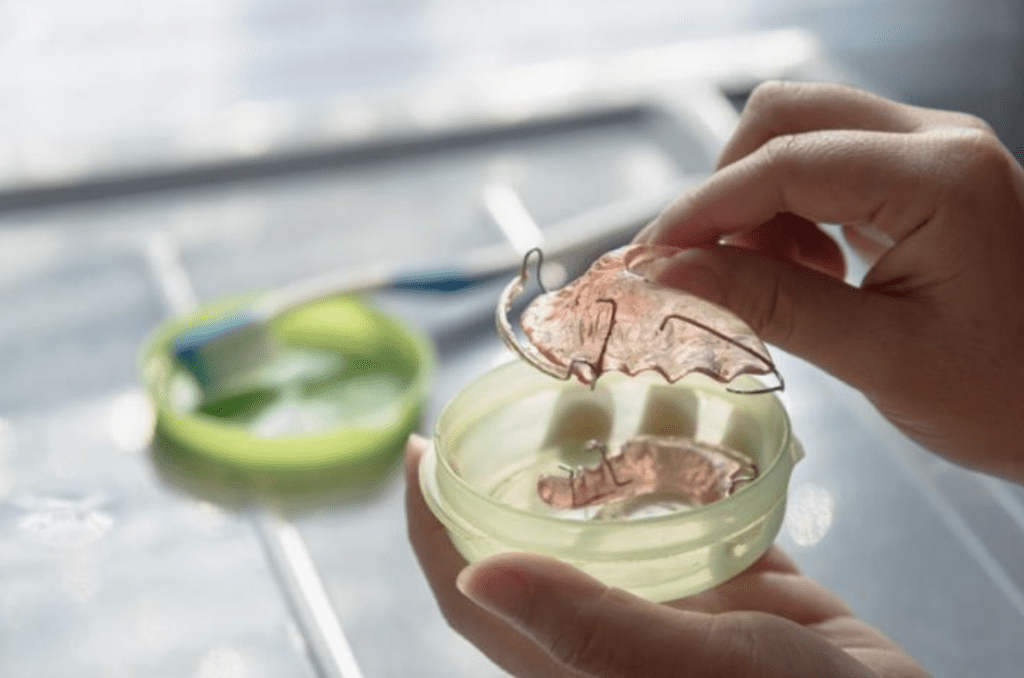
Post-Orthodontic Questions for Retainers
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…

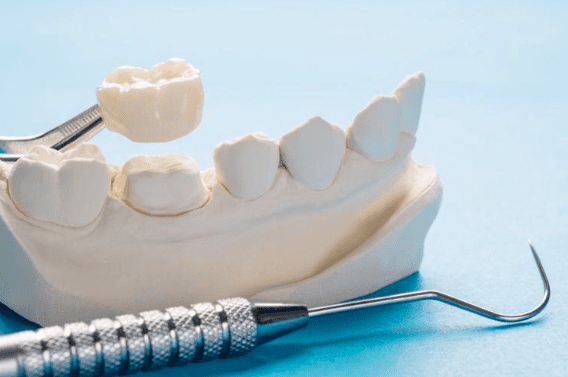
Predictable Veneers: The Art of Shrink Wrap Provisionals
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…
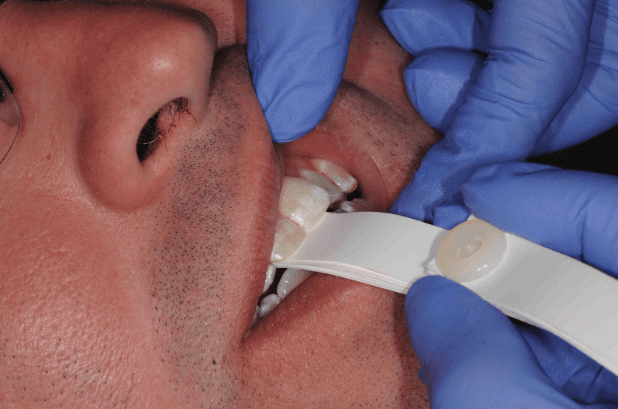
Cracking the Case: Understanding Broken Provisionals
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…
A Dentist’s Perspective on Retainer Wear Time
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org Patients tend to want to spend as little…

Do Patients Parafunction In Centric Relation?
By: Lee Ann Brady DMDArticle Originally Appeared on PankeyGram.org Seated Condylar Position I know even the mention…

My Favorite Occlusal Deprogrammers
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org Deprogramming of the lateral pterygoid muscle is generally done…
When Your Occlusal Clearance Disappears
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org It can be an incredibly frustrating clinical situation…

Occlusal Wear: Is It Advancing? How Fast?
By: Lee Ann Brady DMD I ask the question “Is wear normal?” at almost every lecture I…
Maximize Your Profitability Through Dental Real Estate
It takes a lot to make sure your choice regarding dental real estate is the right one for you, your budget, and your future.
Advice For New Associates in a Dental Practice
Welcome to the world of the business of dentistry. Here’s what you need to know if you’re starting out as a dentist and heading down the path of becoming an associate.
Dealing with Imposter Syndrome in Your Dental Career
By: Amisha Singh, DDS Leadership. You have heard the word, and maybe even understand the importance for your dental practice and your career. But this concept, which supports an industry of educators and thought leaders, remains an enigma for most practitioners. And there is one fundamental reason for this: Leadership in theory and leadership in…
3 Dental Insurance Mistakes Practices Are Making
As we dive deeper into 2021, dental insurance expert Teresa Duncan of Odyssey Management is seeing three big issues with dental insurance that practices encounter.

Advice Every Dental Practice Should Hear: From a Baseball Usher
A bike ride past Tropicana Field in St. Petersburg, Fla., brought back memories of some great advice from an usher for dental practices.

WalletHub unveils 2021 list of best and worst states for dental health
So where does your state rank in terms of dental health for 2021? WalletHub has compiled its annual rankings.

Differences in the Workplace “Garden”
We all have stunning gardens that are unique to each one of us, writes Natalie Kaweckyj. She encourages readers to share their knowledge, expertise and passion, and watch the dynamics bloom.

Great Dental Teams Start With a Great Vision
Dr. Robert Maguire discusses what he has learned about building great dental teams during his years in the dental industry.
Dental Assistant Drama in the Practice: Q & A
One dental assistant is tired of the drama in her practice … but she’s making a plan on how to change her viewpoint.

The one thing that dental team members want more than anything else
There is one thing that your team members want more than anything else in 2021. No, it’s not more money.