
![]()
Dr. Lee Ann Brady lives in Phoenix, Arizona with her husband Kelly and three children Sarah, Jenna and Kyle. She owns Desert Sun Smiles Dental Care, a private restorative practice in Glendale, Arizona. Outside of her private practice, Dr. Brady is the Director of Education for The Pankey Institute, recognized for hands-on education programs focused on occlusion and restorative dentistry. She is the founder and lead curator of Restorative Nation, a supportive learning community for dentists.
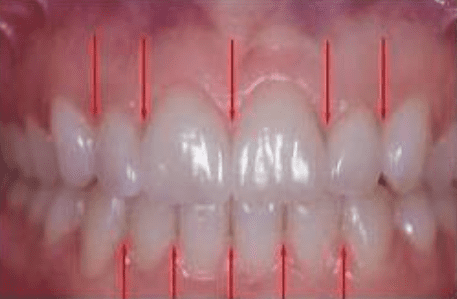
Interdental Papilla: Esthetic Considerations
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…

Post-Orthodontic Questions for Retainers
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…

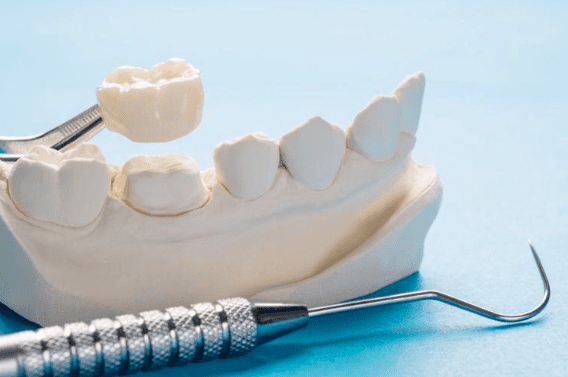
Predictable Veneers: The Art of Shrink Wrap Provisionals
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…
Cracking the Case: Understanding Broken Provisionals
By: Lee Ann Brady DMDTopic originally appeared on Pankey.org: Dr. Brady allowed permission for igniteDDS to share…
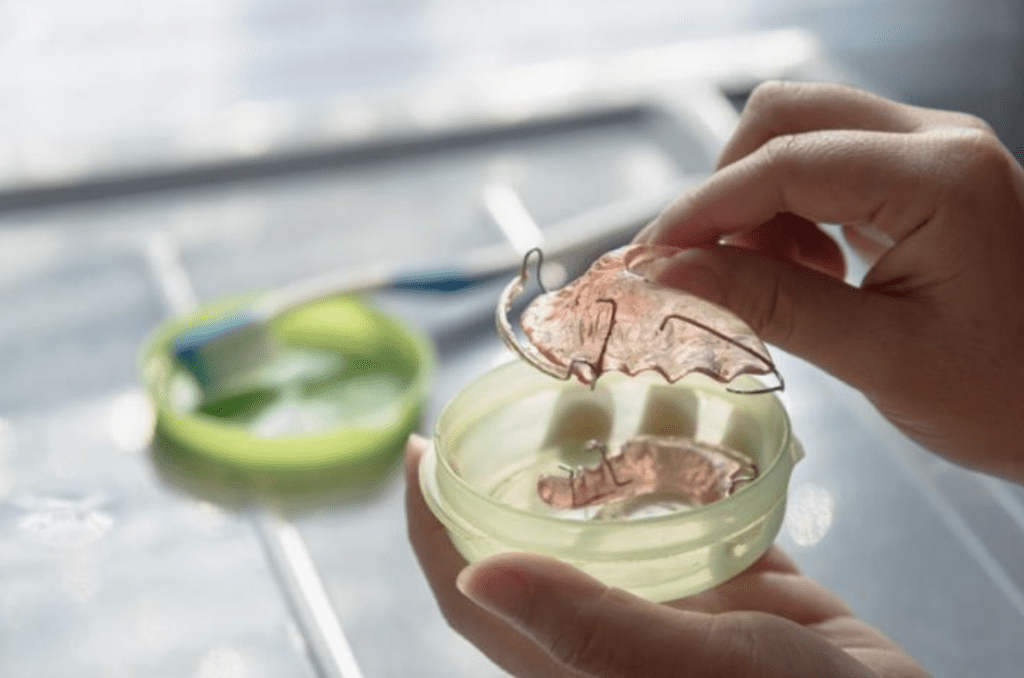
A Dentist’s Perspective on Retainer Wear Time
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org Patients tend to want to spend as little…

Do Patients Parafunction In Centric Relation?
By: Lee Ann Brady DMDArticle Originally Appeared on PankeyGram.org Seated Condylar Position I know even the mention…

My Favorite Occlusal Deprogrammers
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org Deprogramming of the lateral pterygoid muscle is generally done…
When Your Occlusal Clearance Disappears
By: Lee Ann Brady DMDTopic Originally Appeared on PankeyGram.org It can be an incredibly frustrating clinical situation…

Occlusal Wear: Is It Advancing? How Fast?
By: Lee Ann Brady DMD I ask the question “Is wear normal?” at almost every lecture I…

How to Avoid Some of the Biggest Dental Real Estate Mistakes
How can you avoid some of the biggest real estate mistakes when it comes to your dental practice? Ken Jorgenson of CARR.us is here with some advice.

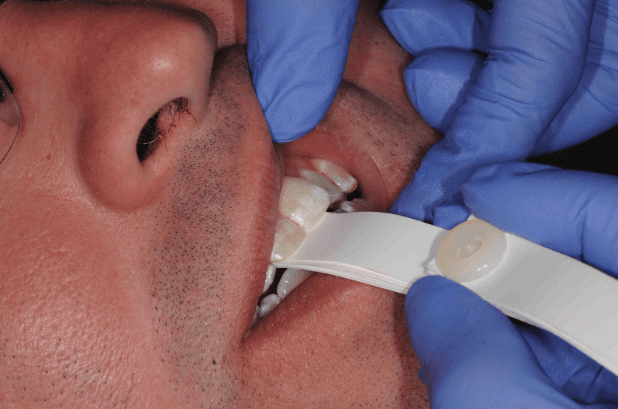
How to Give a Painless AMSA Dental Nerve Block
Giving a painless AMSA nerve block is paramount in any dental esthetic case. It’s also a major efficiency win in treating multiple anterior teeth.
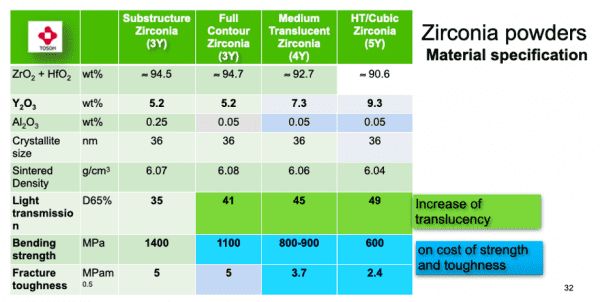
Zirconia: What Your Dental Lab Isn’t Telling You
By: Dr. David Rice As we all know, Zirconia is just one type of dental material at our disposal as dentists today. Do you know what I love about my dental lab? They speak the truth, the whole truth, and everything around the truth. Thank you, Bonadent! I was reminded of that as I spoke…

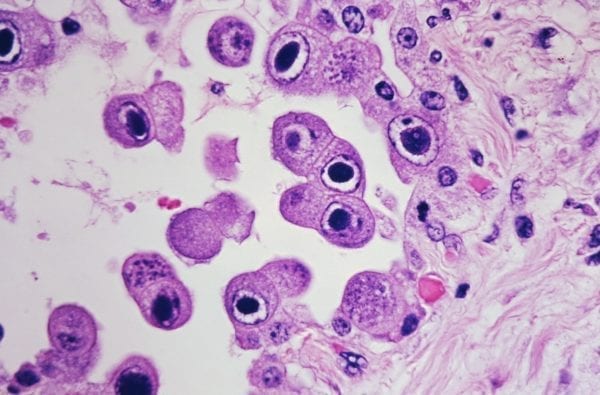
How dentistry helped solve an ancient murder
It’s the stuff that you love to watch on Netflix with the lights turned down. It revolves around a murder mystery from long ago that there were plenty of ideas about, but no concrete proof of exactly what happened and why. There were plenty of guesses and theories, but it took dentistry to crack the…
Maximize your profitability through dental real estate, part 2
In part 2 of this series, we will continue discussing how to maximize your profitability through dental real estate.

Let’s talk Michael Strahan and smile design in your dental practice
Michael Strahan’s dental-related April Fools’ Day joke got us thinking about the options that could be available to him with today’s dental technology.

Lessons Learned from the Pandemic As a Dentist
By: Dr. Bill Simon A career in dentistry can certainly offer up its share of challenges. Some may feel like little bumps in the road, some like speedbumps, and some, hopefully very few, will feel like the road has disappeared. The COVID-19 pandemic caused the road to disappear. As a dentist, you live and you…
Why dental practices need to know about zero click searches
How can zero searches on Google and other sites help your dental practice? Sean Hamel is here to explain.

Embracing Failure to Adopt Everyday Innovation
An important lesson in leadership? Understanding that it’s OK to fail if you’re learning from your mistakes and moving forward.
Infection control: How NOT to get sued … and a whole lot more
Here are three simple questions to answer when it comes to infection control in the dental practice.