
By: James Kohner, DDS
This article originally appeared on PankeyGram.org. Dr. Kohner granted permission for igniteDDS to share with our readers.
The Single Most Important Rule: Bone to Restorative Margin
The cause of most of restorative failures like poorly fitted dental crowns, chronic gingival inflammation, poor impressions, and provisional dental restorations that just won’t stay cemented, is one fundamental principle that dictates soft tissue health when dental restorations are placed: The relationship of the bone to the restorative margin.
This principle is the essence of managing the biologic width, which refers to the height of the supra-crestal attached tissues, such as connective Tissue Attachment (approximately 1.0 mm), epithelial attachment (approx.1.0 mm) and gingival Sulcus (1mm).
This was first established in the 1960s by Gargiulo, Wentz, and Orban as the average dimensions of healthy gingiva (3mm), and serves as clinical guideline.
The Violation & The Consequences
When the restorative margin (the finish line of the dental crown) encroaches into that approximately 2 mm of attached tissue, a phenomenon known as biologic width violation occurs, and the body has only a few unpleasant ways to react:
- Chronic Inflammation: The most common response is a persistent, localized redness, swelling, and bleeding that often gets misdiagnosed as poor patient hygiene, or is mistakenly attributed to an “allergic” reaction to the dental crown materials when it is really mechanical impingement issues.
- Gingival Regrowth: After a simple gingivectomy (cutting away only soft tissue), the gum will almost inevitably grow back to re-establish the 3 mm distance to the nearest bone.
- Localized Bone Loss: In some cases, the body will resort to removing the adjacent bone to create space for the biologic width, leading to unpredictable recession and potential attachment loss.
A healthy dental crown requires the margin to respect the attachment. If clinicians cannot see healthy tooth structure for margin placement, there is a bone problem, not just a gum problem, and this is relevant for any restorative margin placed subgingivally. On the other hand, note that supragingival margin placement is a desirable alternative that avoids these impingement issues.
Crown Lengthening to Improve Restorative Treatment
Crown lengthening is fundamentally a bone contouring procedure that moves the underlying osseous crest apically to expose sound tooth structure, thereby creating the necessary 3 mm distance.
This procedure solves two major categories of common restorative challenges:
1. Retention & Preparation
How often do clinicians struggle to get a clear impression or find that provisionals keep debonding on a posterior tooth?
- The Problem: The short clinical crown height is often due to an excessive amount of bone and attached gingiva covering enamel or coronal root structure, or loss of tooth structure from caries or fractures. One might try to extend the prep subgingival to gain retention, but this only risks violating the biologic width, leading to irritation.
- The Solution: By removing the excessive bone and scalloping it around the tooth, practitioners can dramatically increase the available ferrule and retention height. This allows placement of margins, whether supra-gingival or minimally sub-gingival, on a sound, healthy tooth, ensuring predictable cementation and restoration longevity.

Fig 1. Example of too much soft tissue as a result of too much bone, thus making clear access to the finish lines impossible. Gingivectomy will not solve this problem since it does not recontour the bone.

Fig 2 Three-year post-restoration illustrating healthy soft tissue that follows removal of excess bone and soft tissues. Dental crowns can then be placed without any danger of either biologic width violations or open crown margins due to inadequate impressions failing to capture margins.
2. Marginal Integrity & Finish Lines
When a patient presents a failing, old crown and the classic “ever since I had this crown, my gums hurt” story, the radiograph often holds the key.
- The Problem: Look for a crown that appears too short or evidence of enamel that was never included in the prep.
- The Solution: Crown lengthening allows removal of the soft tissue and bone to reveal more tooth structure and a clean, healthy margin for a new preparation. Clinicians thus gain complete control over the finish line, which is critical for both traditional and digital impressions because one must be able to visualize the margin clearly.
Radiographs: A Great Diagnostic Tool
Clinicians can gain significant diagnostic information without even a clinical exam. When evaluating a radiograph, look for clues that indicate the soft tissue attachment is high up on the tooth, such as:
- Short Clinical Crowns: The height of the crown from the occlusal surface to the margin looks unusually short.
- Enamel Not Included: Significant coronal enamel that the previous restoration failed to incorporate because the gum tissue was in the way.
These indicators are a green light for crown lengthening.
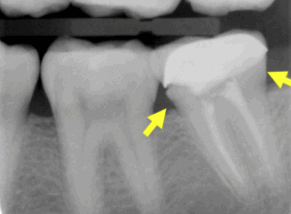
Fig 3 The arrows illustrate open margin mesial, and enamel that was not and most likely should have been included in the prep, both mesial and distal.
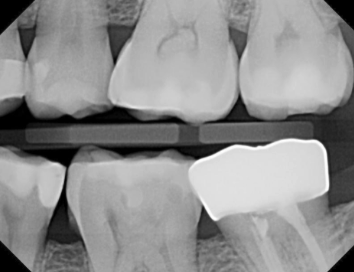
Fig 4. Post op of the same tooth. Removal of bone and soft tissue allowed for proper prep and a restorative result that has better form of prep and crown, and no open or short margins.
Communicating with Patients: The Win-Win Strategy
The last critical step is communication. Never surprise a patient with the need for surgery. When a patient asks for replacement of a failing restoration, adopting this strategy to manage expectations might be a benefit for all:
“Jane, I can certainly make you a better crown. However, based on the age and condition of this existing one, there is a very high chance that the tooth structure needed for a proper crown is covered by gum and bone. If that’s the case, you will likely need a minor surgical shortening of the gum to ensure the new crown is healthy and lasts. I won’t know for sure until I remove the old one.”
This is a win-win for the restorative dentist:
- If surgery is needed, the patient is forewarned and more readily accepts it.
- If surgery is not needed, the patient is pleasantly surprised and appreciates the diagnostic thoroughness of the clinician.
Dentistry has a professional and ethical responsibility to save teeth when possible. By truly understanding and applying the principle of bone to restorative margin, clinicians can transform non-restorable challenges into predictable successes, minimizing the need to reach for the titanium solution.
If you want to learn more about complex surgical and restorative treatment planning to manage similar cases in your clinic effectively, I highly suggest everyone the Mastering Advanced Prosthodontic Techniques – an advanced hands-on course at The Pankey Institute.












