
By: Dr. Anna Babczyńska-Staszewska
This topic originally appeared on dmg-connect.com. Dr. Anna gave permission to igniteDDS to share with our readers. [click to open PDF]
A female patient (age 25) with chalky white opaque areas covering the middle and incisal thirds of upper central incisors was looking for aesthetic treatment. (Fig. 1).

Fig. 1: Initial situation before treatment
A decision was made to treat the lesion using micro-invasive treatment to fulfill the patient’s desire for an aesthetic smile. Bleaching and resin infiltration treatment with Icon (DMG) were proposed.
Preparation of BleachingTrays
The patient’s teeth were scanned with the 3Shape TRIOS 4 intraoral scanner (Fig. 2).

Fig. 2: Scanning with 3Shape TRIOS 4 treatment
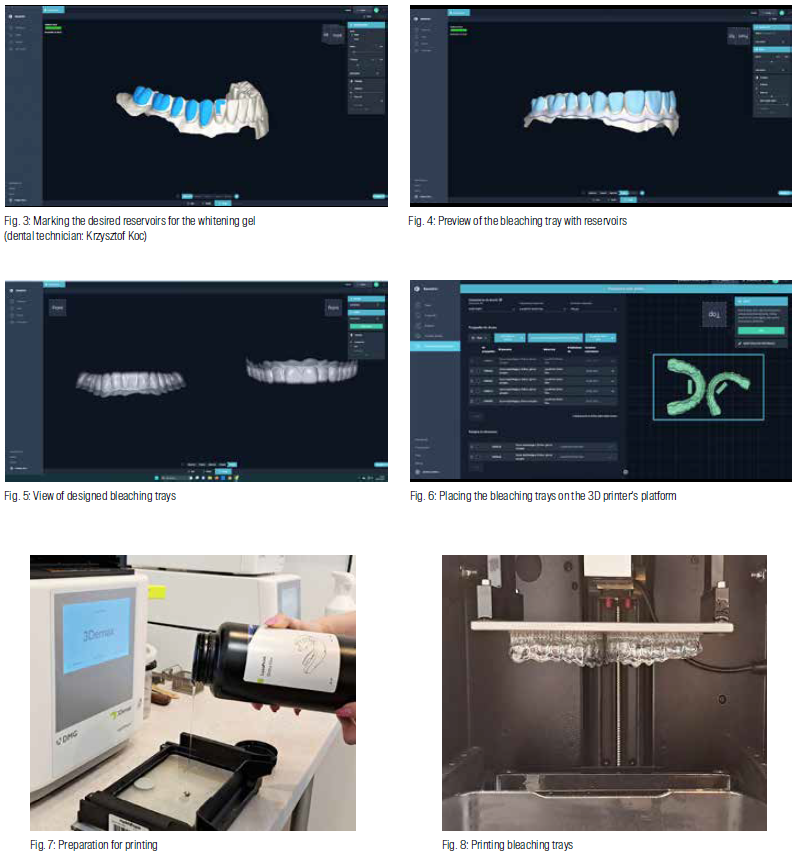
The treatment started with home bleaching using the White Dental Beauty carbamide peroxide (CP) gels. Trays were designed using DMG DentaMile connect CAD software and printed in a DMG 3Demax with LuxaPrint Ortho Flex resin.
The design and printing of bleaching trays are undertaken by a dental technician. The process begins with sending the patient’s STL files via the DentaMile connect platform. Subsequently, the bleaching tray design procedure is initiated at the dental lab, followed by the production of the finalized trays.
The reason why DentaMile connect was chosen for design was because of its user-friendly interface, three-step design process, guided workflow and compatibility with 3D printing. The design’s precision in home bleaching gel minimized gel leakage and gingival irritation. The user-friendly and intuitive handling, along with economic efficiency and time savings, validated its selection. (Fig. 3-8).
Bleaching
Home bleaching lasted five weeks. During the first week, the patient bleached only the upper arch using 10% carbamide peroxide (CP) White Dental Beauty Gel. Subsequently, for the following week, the patient applied a 16% (CP) gel. In the third week, the patient bleached only the lower arch using 10% (CP) gel, and in the fourth week, a 16% (CP) gel was used. In the fifth week, the patient bleached both dental arches simultaneously using a 16% (CP) gel.

Fig. 9: Handing over the bleaching trays to the patient
The patient worethe bleaching tray for eight hours per day. This method, proposed by Professor van Heywood, serves to minimize sensitivity and encourage patient.

Fig. 10: After 5 weeks of bleaching compliance with the bleaching regimen
The patient reported follow-up visits every week (Fig. 9 and 10).
Microabrasion and Resin Infiltration Treatment with Icon Vestibular
Two weeks after the bleaching was completed, further treatment was performed. The final stage of the treatment involved microabrasion and resin infiltration using Icon Vestibular (DMG).
First, a rubber dam was applied to achieve a dry and clean work field. Microabrasion (Opalustre) and air abrasion were performed to clean and smooth the surface and to gain initial access to the porosities (Fig. 11).
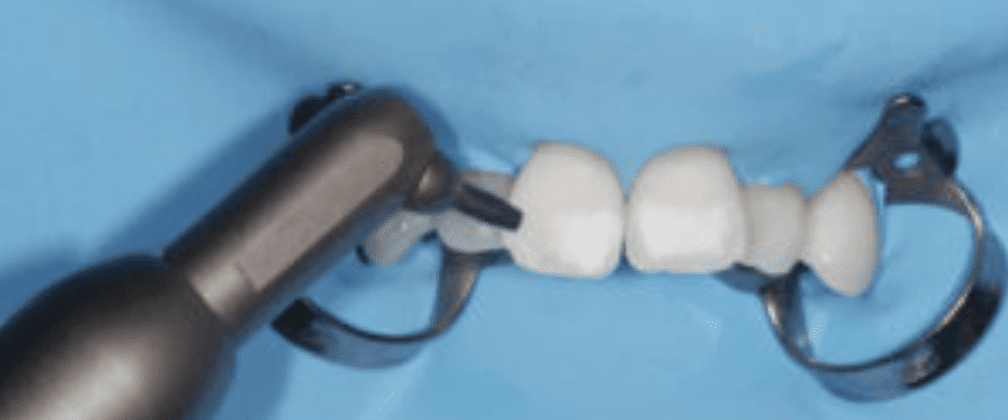
Fig. 11: Microabrasion procedure. Pre-treatment before infiltration with Icon Vestibular (DMG) – air abrasion
Etching with Icon Etch was performed for two minutes, and then Icon Dry was applied. Once the white spots had disappeared after application of Icon Dry, the enamel was ready to be infiltrated. The etching-drying cycle was performed five times. Finally, the Icon Infiltrant was applied in two steps.
The first application was performed for four minutes, with the surface protected from ambient light. The time was extended because no satisfactory effect had been obtained after three minutes. By extending the infiltration time to four minutes, the stain became invisible. Then excess resin was removed, and light curing was performed for 40 seconds (Fig. 12).

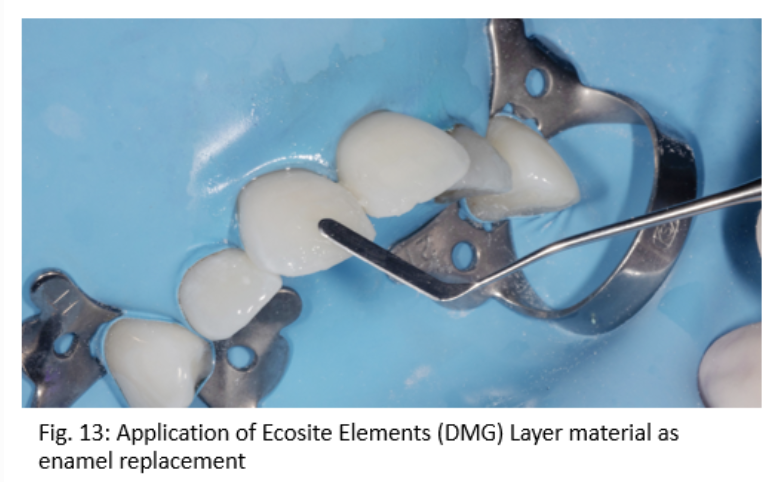
The loss of substance of enamel due to the combination of microabrasion and acid erosion was restored with Ecosite Elements Layer EL composite material. The shade was selected at the beginning of the visit, before placing the rubber dam (Fig. 13).
Finishing and polishing were performed with the Profin® Reciprocating System and EVE DIACOMP® PLUS TWIST. Transillumination using white light was performed to check how effective the method had been.
Conclusion
The incorporation of the DMG bleaching tray workflow further reinforces the effectiveness of the treatment. This workflow ensures superior results by providing a precise bleaching gel reservoir, preventing gel leakage and avoiding gingival irritation.
Additionally, the absence of model preparation and thermoforming significantly streamlines the process, eliminating a considerable portion of both labor and material costs.
Furthermore, it is worth noting that the patient’s positive experience with wearing the bleaching tray – marked by the absence of hypersensitivity or gum irritation – attests to the comfort and success of this approach. (Fig. 14).
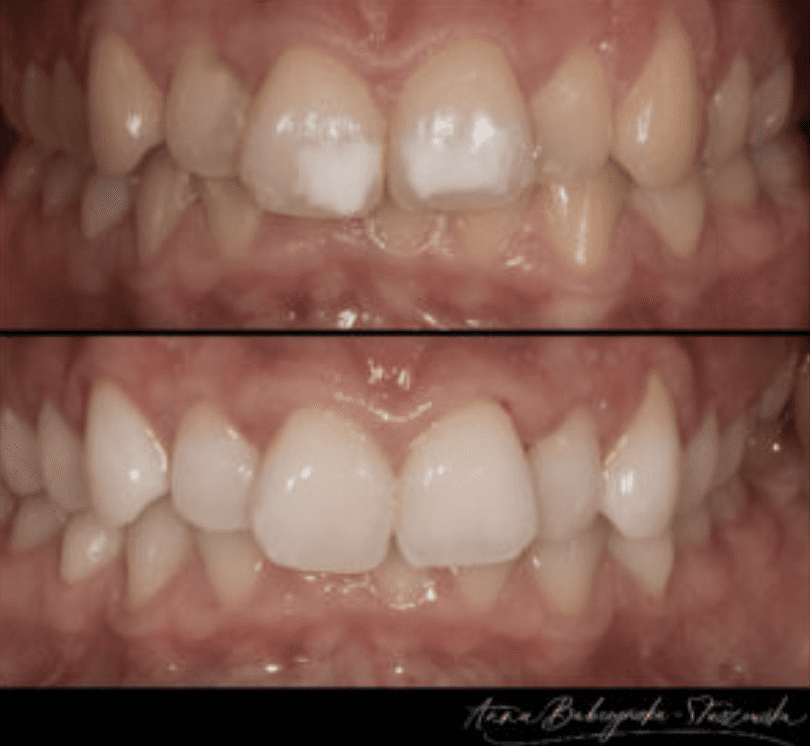
Fig. 14: Before and After












