
By: Jeffrey W. Horowitz, DMD, FAGD, D-ABDSM, D-ASBA
A scalloped tongue is characterized by wavy or rippled edges along its sides.
Scalloped tongues are usually not a cause of concern, but if left untreated, they can cause additional complications and symptoms that can harm your dental health.
Identifying bad oral habits and diagnosing certain medical conditions may also be made easier by a scalloped tongue.
Scalloped Tongue: Case Study
Let’s look over a case study from a patient I had with a scalloped tongue to help you in your diagnosis and treatment with future patients.
Patient Information:
- 38-year-old white male presents for an initial dental exam
- Medical history is positive for hypertension and G.E.R.D.
- Dental/Perio Exam negative for pathology
- Archform is narrow with a high palatal vault
- Soft tissue exam positive for oro pharyngeal inflammation/edema

3 Primary Reasons for Tongue Scalloping
- A Large Tongue (Macroglossia)
- Small Dental Arches / Malposed Teeth (may be developmental or iatrogenic)
- A Combination of the Above
These patients are at higher risk for airway obstruction and further assessment of the airway is indicated.

Narrow Arches, High Palatal Vault
- The tongue may be normal in size but forced to function within an undersized dental/skeletal archform.
- Archforms may be underdeveloped from poor tongue posturing during childhood/adolescence. This is often initiated by early airway insufficiency.
- Archforms may be undersized by reductive orthodontic therapies (Extraction/IPR) to correct crowding or through space closure

Big Tongues; The Tongue Level Can Be Graded
Type 1 – Tongue at rest with lateral border BELOW mandibular occlusal plane
Type 2 – Tongue at rest with lateral borders LEVEL WITH mandibular occlusal plane
Type 3 – Tongue at rest with lateral borders RESTING ON occlusal surfaces of mandibular teeth
Type 4 – Tongue at rest with lateral border COVERING ENTIRE occlusal surfaces of mandibular teeth
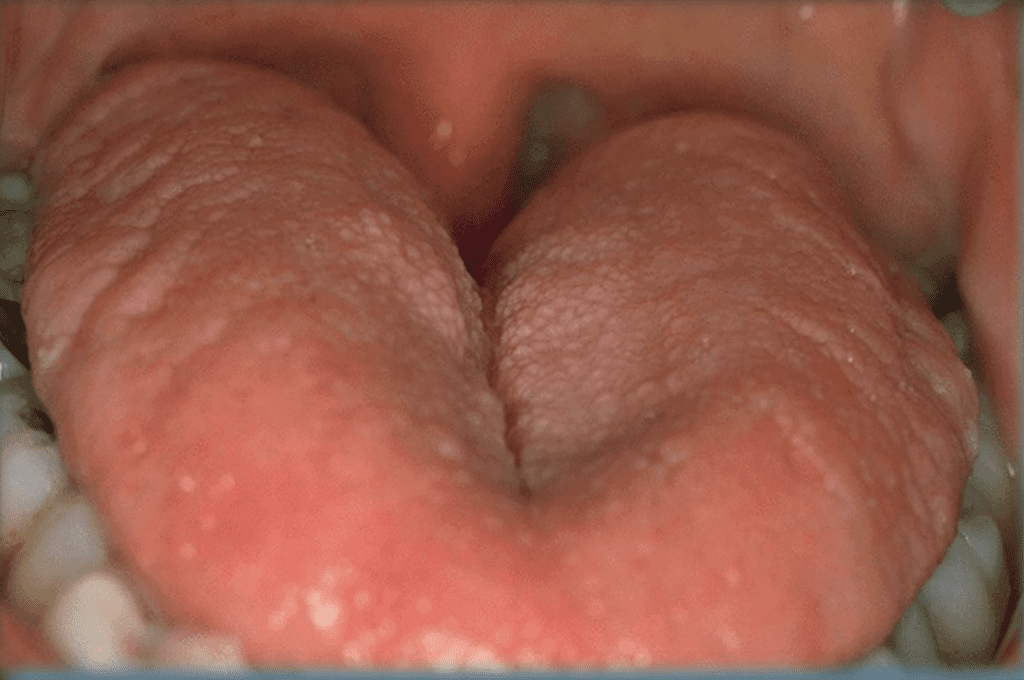
Pictured Above: Tongue Level 3 as tongue at rest covers occlusal surfaces of lower molars without fully covering the occlusal surfaces (type4). Type 3 and Type 4 tongues are risk factors for sleep-disordered breathing.
Compromised Tongue Space Can Lead To A Compromised Airway!
Further airway assessment is indicated to include the evaluation of other oro-pharyngeal structures. (soft palate, lateral pharyngeal walls, uvula, tonsils, and skeletal patterns.
Subjective questioning for snoring, gasping, sleep quality, and daytime sleepiness should be considered.
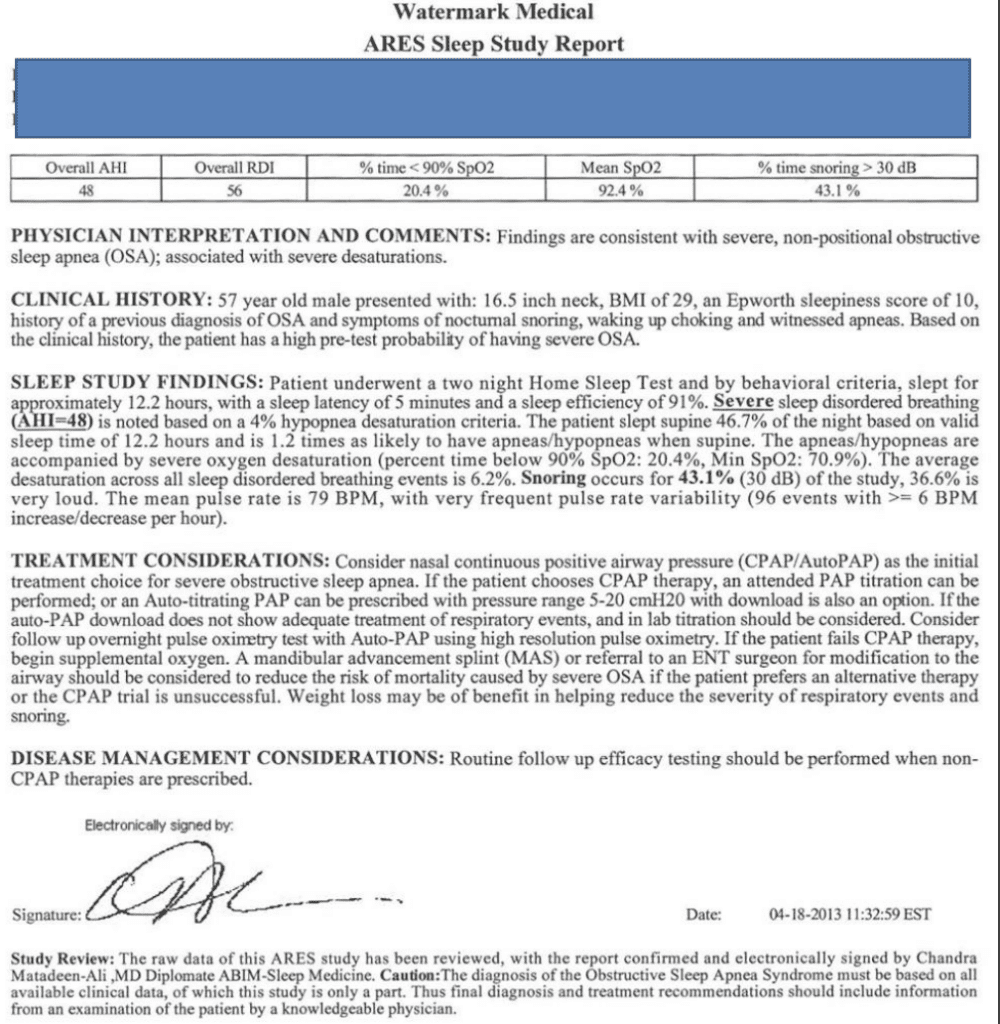
With any concern for airway disorders, referral to a well-trained sleep physician/dentist can lead to reduced medical risk and save lives. Once a sleep study is performed, sleep-disordered breathing can be confirmed or ruled out.
In Summary
The patient was confirmed to have severe sleep apnea after a home sleep study was diagnosed by a board-certified sleep physician.
The patient was successfully treated with a Mandibular Repositioning Appliance
A scalloped tongue is just one of many anatomic presentations that can easily be recognized by dental professionals as a risk factor for sleep-disordered breathing.
NEXT READ: The Importance of an Infection Control Coordinator
Photo by Andrea Piacquadio












